The long-term effects of COVID

Sometimes things just work out a particular way. Two days ago I got the bivalent COVID vaccine and that same day Nature Medicine released a new paper on the long-term effects of COVID infection. The paper has already been getting a lot of attention and as you would imagine people are quickly trying to downplay the implications, because the facts are not looking good to those who want to minimize COVID. In fact, at this point ignoring the dangers is ignoring reality and sadly people seem to be okay with pushing that ignorance. So let’s talk COVID… again.
COVID is not the flu, it’s not a cold, it’s not any of those things. SARS-CoV-2 or COVID-19 for the rest of us is unique to itself. Actually, it’s closely related to its sister SARS-CoV-1 and if you’re over the age of 25-ish you may recall that in 2002-2004 (again -ish) there was a serious concern that it there would be a pandemic level event. Thankfully the difference between SARS-CoV-1 and SARS-CoV-2 was that CoV-1 symptom onset was rapid, so containment happened quickly. This was not the case for CoV-2 and it shows.
The time from infection to symptoms for SARS-CoV-1 was anywhere from 2-14 days, that was key to why we it didn’t become a pandemic. Between the swift response and the short time between infection and symptoms we (the world) were able to contain it and as usual people downplayed the people worried about a pandemic saying they were concerned over nothing. This would be amplified again when SARS-CoV-2 first hit and is still ongoing between people saying there isn’t a real pandemic, that the pandemic is now over, that people aren’t really dying, or that the vaccines are the problem.
The time from infection to symptoms SARS-CoV-2 was anywhere from 7-14 days after infection, while peak viral load was roughly 4-5 days into infection meaning it was far easier to spread and the people spreading it didn’t appear to be infected (in most cases, there’s always people who either were forced to work knowingly sick or the random person who didn’t care about infecting others). Scientists have been sounding the alarm since SARS-CoV-1 because it was only a matter of time before we had another potential pandemic on our hands.
What does this have to do with the study?
Well everything frankly. Thanks to our (scientists) experience with SARS-CoV-1 we knew this was going to be bad, hell there are literal movies that basically gave a play by play of exactly what happened this time. Contagion (released in 2011) was based on this exact eventuality. It was a matter of time and of course people reacted the way we would expect, because this isn’t the first pandemic (1918 flu pandemic for example) and it’s not the first time people with a lot of money and not a lot of integrity are fighting against the things that would keep people safe and alive in favor of profit.
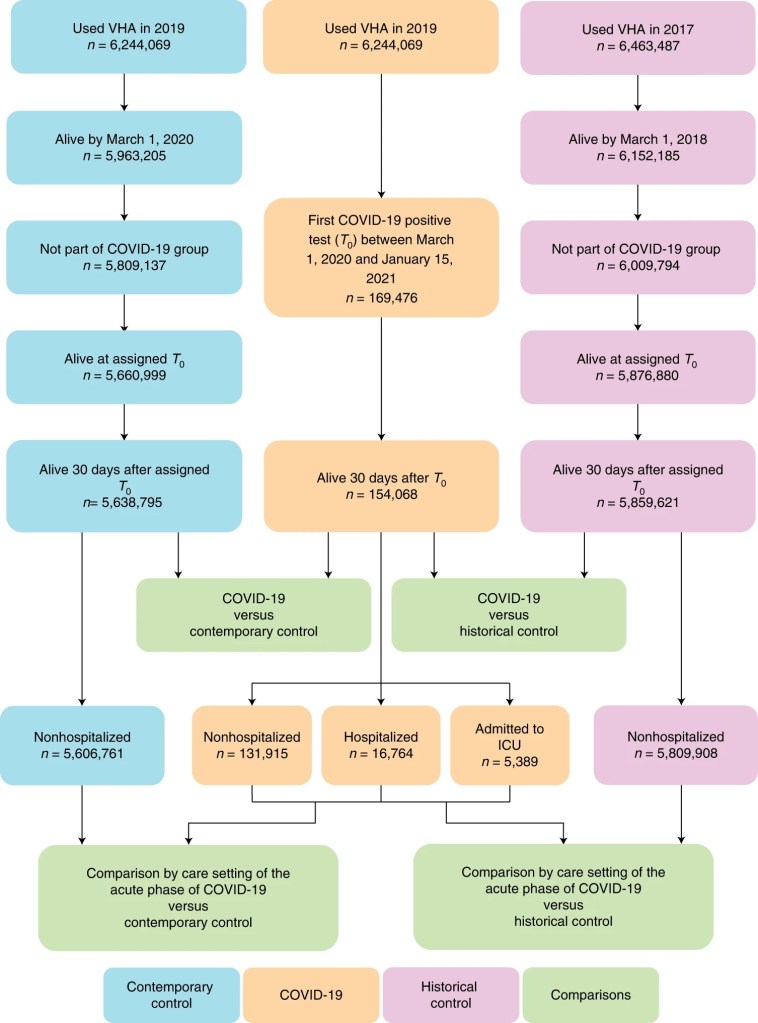
So the study. It was a massive effort (which is why it’s published in Nature no doubt) that I would guess took years of work and effort to make happen. They used the VA (veterans affairs, because veterans in the US are guinea pigs generally speaking) data to track a cohort of 154,068 individuals with COVID-19, 5,638,795 contemporary controls and 5,859,621 historical controls. They define historical controls and data from people prior to pandemic and contemporary controls as data from people who were living through the pandemic and at the time of the study did had not been infected with COVID.
They looked at neurological outcomes 12 months after infection and compared the rate of positives i.e., the things like ischemic and hemorrhagic stroke, cognition and memory disorders, peripheral nervous system disorders, episodic disorders (for example, migraine and seizures), extrapyramidal and movement disorders, mental health disorders, musculoskeletal disorders, sensory disorders, Guillain–Barré syndrome, and encephalitis or encephalopathy, to the control groups.
This is important because there should be a “base” rate for finding those things in the general population so this is comparing to historical data and data taken during the pandemic to control for things like stress because of say, a pandemic. In my opinion this was a great choice because it controls for the rate of these symptoms due to the stresses surrounding the pandemic and also gives us a comparison between historical data and the “pandemic stress” period which is an interesting comparison in and of itself.
Key thing to note! The study did not look at the effect of vaccination on hospitalization or long-COVID, mostly because that’s a different study and has already been done, again and again. People in the anti-vax camp and the “COVID isn’t bad camp” are freaking out over this fact, but that’s because they can’t read. The study is using data PRIOR to the widespread vaccine rollout, specifically data from March 1, 2020 to January 15, 2021. They estimate at most 1% of the contemporary control group to be vaccinated or a non-significant amount that would have skewed the data to the null hypothesis (a null refresher) meaning it would cause a false-negative if anything. They created a very nice flowchart showing how the groups were created (fig 1 from the study).
The news isn’t good.
The study does a great job of outlining how bad the news is, but let’s bullet point it for the people who don’t like reading or don’t have time to read the full study. These are going to be quotes taken directly from the study, if I add clarifying changes or commentary they will be in italics and probably parentheses.
The study found:
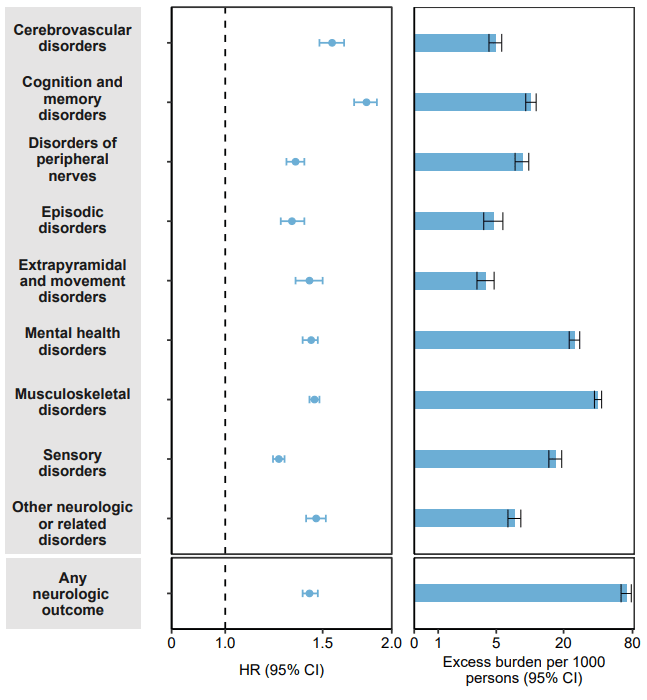
- The risk and burden of a composite of these cerebrovascular outcomes were (HR)1.56 (1.48, 1.64) and (burden) 4.92 (4.26, 5.62), respectively (per 1,000 persons at 12 months where HR is hazard ratio)
- The risk and burden of a composite of these cognition and memory outcomes were 1.80 (1.71, 1.88) and 10.35 (9.27, 11.47), respectively.
- The respective risk and burden of a composite of these disorders of peripheral nerves were 1.34 (1.29, 1.39) and 8.64 (7.44, 9.87).
- The risk and burden of a composite of these episodic disorders were 1.32 (1.26, 1.39) and 4.75 (3.79, 5.76), respectively.
- The respective risk and burden of a composite of these extrapyramidal and movement disorders were 1.42 (1.34, 1.50) and 3.98 (3.24, 4.77).
- The respective risk and burden of a composite of these mental health disorders were 1.43 (1.38, 1.47) and 25.00 (22.40, 27.69).
The list goes on, this was just a small sample of the increased risks that they looked at. They have a good figure for this as well.
Importantly, I think this paragraph sums up the findings:
We then examined the risk and burden of having any neurologic outcome (defined as the occurrence of any incident prespecified neurologic outcome included in this study). Compared with the contemporary control group, there was increased risk and burden of any neurologic outcome (HR 1.42 (1.38, 1.47); burden 70.69 (63.54, 78.01)), respectively.
For those unaware that’s a risk increase of 42% and translates into a roughly 7/100 or 7% chance that if you’re infected with COVID, it will lead to one (or more) of the neurologic outcomes they looked at. That’s higher than your chances of dying in a car crash (~1%), dying in a plane crash (0.00001%), dying from the flu (0.002%), odds of dying from pneumonia (0.0144%), I can’t even find statistics for death from the common cold, need I go on?
Furthermore, the study shows that the risks developing these long-term consequences were evident even among people who were not hospitalized during the acute phase of COVID-19 infection. This means that even mild infection can lead to these outcomes. These risks were evident regardless of age, race, sex, and health characteristics. So, and I write this with the utmost disdain for people who do this, don’t blame disabled people or elderly for this outcome.
Overall, this study adds significant support to other studies showing similar outcomes and they’ve done it in a way that makes it easy to validate. The problem is tracking. COVID numbers are being undercounted, especially now that the US has stopped free testing and tracking. COVID death numbers are being undercounted (as seen again and again). The data are being hidden or taken, depending on who you ask this is done intentionally to make things look “not as bad.” After all, the pandemic was recently declared over by Biden, let’s just ignore the ~500 official deaths per day from COVID.
But this study highlights something we are ignoring even more than the deaths and that’s death is not the only metric. Sure death is bad, we should strive to drive the death rate of COVID to zero or damned near close to it, anything else is a failure and we as a society are to blame, but so are the people in charge of making sure we’re safe. This study highlights the forgotten metrics of disability. There’s going to be entire generations of people who will have to live with this failure, possibly for the rest of their lives.
In short, death isn’t the only metric. If you’ve never been disabled, I don’t recommend it, trust me when I say no one cares outside of the disabled community and people pushing for others to care. You will not find support, you will not find ease of care, not in the US anyway. So get vaccinated, wear the damn mask, and do your part to end the pandemic.
If you don’t odds are, you’ll regret it.
Source:
Xu, E., Xie, Y. & Al-Aly, Z. Long-term neurologic outcomes of COVID-19. Nat Med (2022). https://doi.org/10.1038/s41591-022-02001-z



This is one reason why I don’t feel bad about my decision to get the first two vaccine doses, and why I would not want anybody to use my (rare) autoimmune neuropathy as an excuse to claim the vaccine is worse than the disease. If I’d caught the actual virus while unvaccinated, the result could’ve been exactly the same – with the added impacts of an unbridled contagious illness trying to damage my lungs and other organs. (I had similar neuropathy symptoms during and after a bad flu many years ago. But they were milder that time around, so I never got properly diagnosed.)
Which also means that, though my neurologist recommended that I personally should not get any further booster shots, I should not be catching COVID either! It’s possible that the autoimmune rampage has burned itself out and further exposure to the spike protein wouldn’t do anything … or it might trigger a relapse and pile on more nerve damage. I don’t know and I don’t want to find out. Everybody pleeeease get vaccinated if you don’t have a known contraindication, and try to get this disease out of circulation.
Despite having a rare reaction, I’m still lucky: it was never bad enough to render me unable to work, and I’ve recovered well. A whole lot of people who caught COVID-19 have done worse. We need to get it under control.
LikeLiked by 1 person
September 24, 2022 at 3:31 pm
Thank you for sharing your story! We definitely need to help protect the most vulnerable instead of worrying only about ourselves.
I’m happy to hear you managed to get two doses at least, it’s better than nothing should you come into contact with COVID. I wish you hadn’t had such a severe reaction to it. It’s a shame the immune system has to be so complicated, but maybe that’s also a good thing.
I agree, we do need to get this under control.
LikeLiked by 2 people
September 25, 2022 at 11:56 am