Know your spinal cord – Central cord syndrome
Welcome to day twenty two in the knowing your spinal cord series! As per my usual intro, you can find the rest of the series in reverse chronological order under our spiffy new neuroanatomy category. Today we are covering another type of spinal cord injury, like the last two posts, this will cover what happens when a certain area (central area) of the cord is damaged. With that, let’s talk spinal cord.
Keeping with the theme, the past two posts have been on incomplete lesions of the spinal cord. A lesion being some sort of tissue damage, this can happen from blood flow restriction, illness, or even injury. Today we are looking at central cord syndrome. As the name implies the damage to the cord is centrally located. Below is our somewhat familiar image showing the three major types of incomplete lesions, with central cord syndrome on the top. Just a reminder, we’ve already covered anterior cord syndrome and Brown-Sequard syndrome.
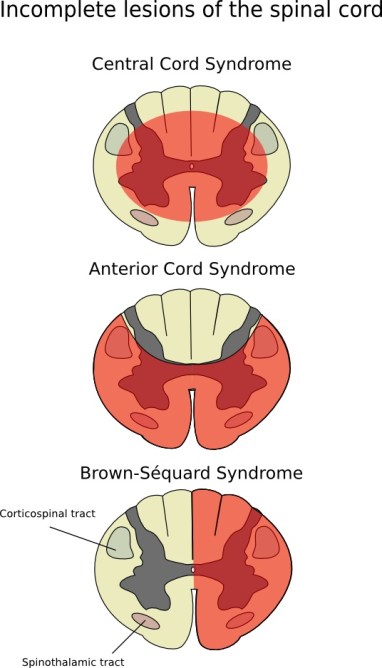
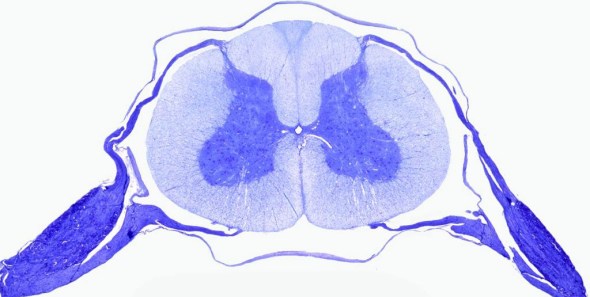
As you can see from the image above, central cord syndrome happens centrally in the spinal cord leaving the outer tissues/tracts intact. Now, if you didn’t know anything about the spinal cord you might think that this would be a rare type of injury, after all how do you injure the center of the cord without damaging the outer tissues? Unfortunately this is not the case. In fact, this is the most common type of incomplete spinal cord injury and accounts for almost 10% of traumatic spinal cord injury. Below is an MRI scan where I’ve highlighted (white circle) what a central cord injury looks like.

Sagittal view of acute traumatic non-hemorrhagic central cord syndrome. I’ve highlighted the damage with the white circle to make it easier to see
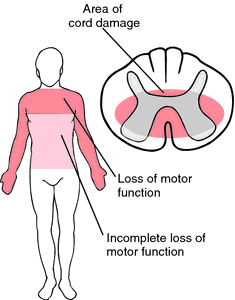
This type of injury occurs in the cervical region of the spinal cord and is characterized by loss of control and sensation of the arms and hands. There is also variable degree of sensory loss below the level of injury in combination with bladder dysfunction and urinary retention, which is a common problem in the spinal cord injury population. As you might suspect, it usually results from trauma that damages the neck, which then causes major injury to the central corticospinal tract. Below is an image showing the overview of the loss of function, note that while the lower limbs look to be intact here, the level of function depends on the extent of damage.
This doesn’t just happen from a traumatic injury however. As we get older, our bones begin to weaken, cartilage wears down, and you can be more susceptible to this. For that reason, central cord syndrome is more common in people over the age of 50 because they are at higher risk for cervical spondylosis. Spondylosis is degenerative changes in the spine such as bone spurs and degenerating intervertebral discs between the vertebrae, so cervical spondylosis is degeneration in the cervical area of the spine. However there is a caveat, this happens at a higher rate in older people. Central cord syndrome can and does happen in younger individuals as well. Just a reminder, the spinal cord moves quite a bit as you move around and below is an animated gif showing spinal cord movement from neck flexion and extension.
Look close to the brainstem and you can clearly see the cord move as the neck moves.
As with any spinal cord injury, the prognosis is grim. This is due in part to the mechanisms causing the damage. Historically, spinal cord damage was believed to originate from concussion or contusion of the cord causing edematous injury, or injury due to the swelling of the tissues rather than destructive hematomyelia (spinal cord hemorrhage).
Unfortunately, recent autopsy studies have shown that central cord syndrome may be caused by bleeding into the central part of the cord. Researchers have also found from postmortem evaluation that central cord syndrome is associated with selective axonal disruption in the lateral columns at the level of the injury to the spinal cord with relative preservation of the grey matter. This damage means that while the neural circuitry (grey matter) remains undamaged, the signaling pathways are what is broken. This makes it harder for the spinal cord to compensate.
Once again, first line treatment is a combination of occupational therapy and physical therapy. For those who don’t know the difference, occupational therapy puts the focus on being able to perform day to day tasks, while physical therapy focuses on being able to perform movements. Depending on the extent of the damage, a person with central cord syndrome can still live a relatively normal life. Surgical intervention is sometimes indicated. However, this is typically done to prevent further damage and is unlikely to improve the overall outcome for the individual.
That about wraps up our look at the lesions of the spinal cord. Usually I don’t know what I will be covering the next day. This time however I do know! We will be covering something called Lichtheim’s disease. There are still a few different spinal cord disorders I want to cover, then we might be diving back into some of the smaller tracts of the spinal cord along with some of the anatomy details we haven’t talked about yet. Basically what I am saying is that we will definitely get a months worth of information about the spinal cord, probably a little more before we wrap up knowing your spinal cord.
Until next time, don’t stop learning!



But enough about us, what about you?