Know your spinal cord – Transcutaneous spinal direct current stimulation
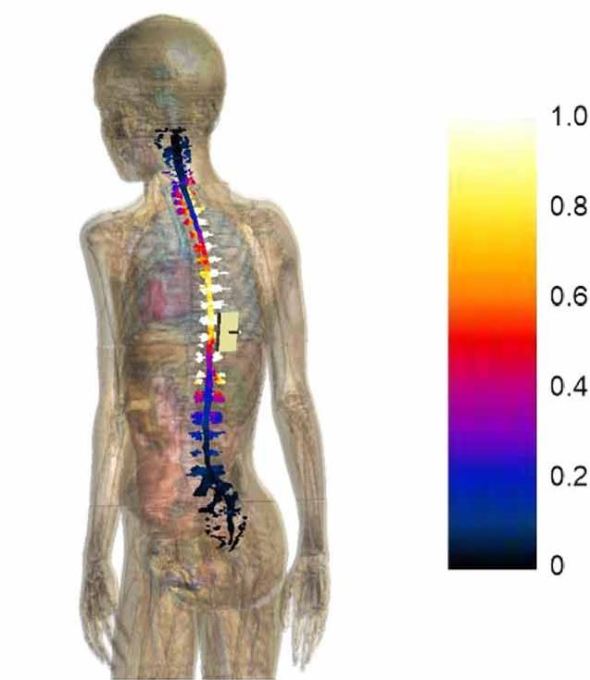
E amplitude distribution over the spinal cord and nerve surface. The color scale on the right is normalized with respect to the maximum of E amplitude in the spinal cord.
Well after our short break yesterday with my biweekly review paper, it’s back to the know your spinal cord series and we’re on day fifty-two! If you’re here for the first time, you can find the posts in this mini-series in the neuroanatomy category. We’ve taken a few twists and turns since we’ve started the series, but we’ve covered way more than I originally planned. We’ve covered how transcutaneous spinal cord stimulation is thought to work, that post focused on the type of spinal cord stimulation I’m researching. However, there are other ways to stimulate the cord. Transcutaneous spinal direct current stimulation (tsDCS) is a different way to stimulate and today we will talk about the difference.
Transcutaneous spinal cord stimulation (TSS) has two rather broad categories, the first is the way we do things in our lab, which is pulsed stimulation. Depending on the task (tonic, ie standing vs. rhythmic ie walking) we stimulate at two different frequencies 15Hz and 30Hz, which depending on who you are talking to is high frequency or low frequency stimulation. There are stimulation paradigms that use much higher frequencies, but that is typically epidural spinal stimulation. We stimulate at (broadly speaking since it is VERY person specific) 40-60 mA, that is important because this is how we create the motor response you’ve seen in the video we’ve shared. We also use a biphasic stimulation pulse (the end of the pulse is negatively charged) to avoid charge buildup at the pad. Below is an image showing different waveforms to show what a biphasic waveform looks like. We use an 20% asymmetric waveform meaning the last 20% of the pulse is negative.
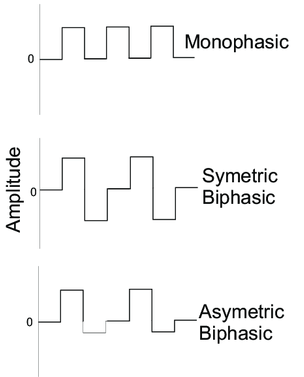
Monophasic (top), symmetric biphasic (middle), and asymmetric biphasic (bottom) waveforms are different ways we can stimulate. The bottom appears to have an asymmetric amplitude, in our work the amplitude is the same, but the pulse width is what we change.
The second category is direct current stimulation (tsDCS), we just did a review on the topic yesterday (hence today’s post). Direct current stimulation is different and distinct from pulsed stimulation because the current delivered is a constant monophasic (all positive) stimulation. The stimulation intensity is also much lower at around ~2.5 mA, which is far lower. So low in fact if we stimulated (pulsed) at that intensity, the person would typically not even feel it. Below is an image showing the typical placement of the electrodes, you’ll notice that this is basically the same setup we use for pulsed stimulation.
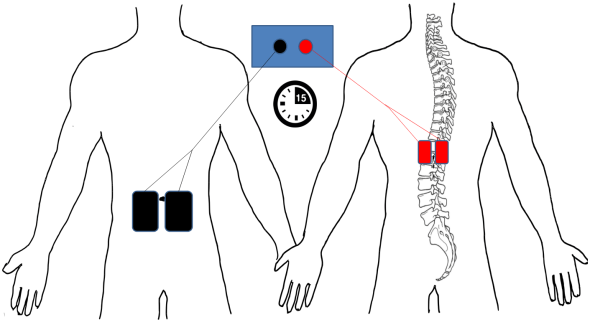
Electrode montage for tsDCS. The bifurcated anode (red) is placed centrally and paravertebrally over T11, T12 thoracic vertebrae and the bifurcated cathode (black) is placed centrally and lateral to the umbilicus. 2.5 mA of anodal direct current was applied for 15 minutes, providing 0.0833 mA/cm2 current density and 0.075 C/cm2 of total current applied DOI: 10.1371/journal.pone.0173846
Direct current stimulation is currently more of a neuromodulation tool and not a rehabilitation tool. It is just another way we can “poke” the spinal cord and see how the networks react to the stimulus. When applied to the brain (transcranial direct current stimulation) we find higher cortical excitability, an effect that lasts long after the stimulus is removed. If we could determine why this occurs or how to maintain this higher excitability it would be advantageous.
However, that is really all this type of spinal stimulation can do, there is little (almost no) evidence to support that it increases motor function significantly, which is why we used pulsed stimulation in our lab. That doesn’t mean it isn’t an important tool in understanding the spinal cord, it just means that like every tool it has very specific things can and cannot do.
Hopefully that is a good introduction to tsDCS and why we use a pulsed stimulation in our lab over a constant current stimulation. Some of you may be wondering why we stimulate at 15 Hz or 30 Hz and the answer is not very scientific. It’s the frequency that seems to give the best result, seriously. We are trying to figure out the secrets of the spinal cord, but unfortunately we are still very much groping around in a dark room looking for a flashlight.
Next, up? Well that depends, but with the coronapocalypse upon us, I’m not sure since day to day things are changing very rapidly (experiment and school wise). Here’s the obligatory PDA straight from the labs. Stay safe, practice social distancing, wash your hands, and don’t touch your face. Even if you are healthy, you need to practice these things, you could become a vector and get people sick who are not healthy, don’t be that person. We’ll get through this together. In the meantime, this blog has been going for sometime now so we have a long selection of posts for your science reading enjoyment!
Until next time, don’t stop learning!



But enough about us, what about you?