Know your spinal cord – Transcutaneous Spinal Stimulation
Welcome to day forty-four in the know your spinal cord series! As usual all of our posts are in a super easy to find neuroanatomy category. Now that we’ve covered our into into diagnostic tools to probe the spinal cord, let’s look at some of the ways we are working to help treat spinal cord injuries. Today we’re looking at a heavy hitter so to speak and something my research is focused on, transcutaneous spinal stimulation (TSS). Let’s take a look!
I’m really excited for today’s conversation. Transcutaneous spinal stimulation is cutting edge work that is being researched to help treat spinal cord injury. There is only a handful of people in the world doing the research and we aren’t quite sure what the limitations are or even what exactly we are stimulating. We know it works, and we’re trying to figure out how exactly it does that, but it’s a work in progress.
Spinal cord stimulation currently comes in two flavors so to speak. One is TSS, that is my focus. The other is epidural spinal cord stimulation, this is an invasive type of spinal cord stimulation though so electrodes are inserted into the epidural space. Let’s look at what exactly is done when we are talking epidural spinal stimulation so we can see the differences. Below is an image showing the placement of the electrodes (in an X-ray, left), where exactly the electrode is placed (right), and what the system looks like (center).

Epidural spinal cord stimulation setup showing the electrode inserted into the epidural space and the implanted battery pack (left), the electrode array and battery pack itself (center), and where the electrode array is placed in terms of the spinal cord (right)
As you can imagine, surgery can make this very inaccessible to people and worse, because you need surgery they only place these electrodes as indicated, so we cannot place this ethically into a healthy subject for example to test its effect on healthy populations. This is the gap TSS fills, it let’s us to do research with healthy subjects because it is non-invasive. There is some discomfort associated with TSS, but that is very subject dependent, I’ve seen people laugh because it feels funny to them and I’ve seen people have to stop because they weren’t comfortable with the sensation, it just depends on the person really.
That leads us to how we can stimulate the spinal cord. After all, it’s not out in the open like your muscles are, it’s tucked away inside a column of bones. Below is an image showing how stimulation (is thought to be) applied to the spinal cord.
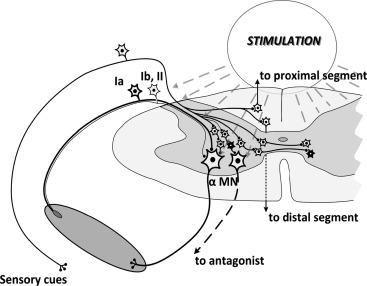
Stimulation is applied to the back and stimulates the entire area of the cord, it isn’t as precise as epidural spinal stimulation, but there are several benefits to this approach.
This works because the Type 1a afferents are easy to stimulate. When we apply a stimulus, it reduces the threshold for the circuitry to fire. When we are working with a spinal cord injury (SCI) population, it is assumed that the damage to the cord makes it more difficult for the volitional signal to activate the circuitry. Therefore, by applying a constant stimulus (depending on the activity, we stimulate at either 15 Hz or 30 Hz) the threshold to fire is lowered, so this reduced amplitude volitional signal creates a larger response. Below we see the response to spinal cord stimulation recorded at a particular muscle.
B.) Transcutaneous stimulation of the lumbar spinal cord elicits posterior root-muscle (PRM) reflexes in multiple lower-limb muscle groups bilaterally. Stimulus-triggered, superimposed representation of 3 consecutive PRM reflexes elicited in right (R) and left (L) quadriceps (Q), hamstrings (Ham), tibialis anterior (TA), and triceps surae (TS) of an individual with chronic incomplete spinal cord injury. Black arrows indicate times of stimulus application. C.) The stimulation of afferent fibers can be verified by testing the recovery cycle of the evoked responses using double-stimuli at varying interstimulus intervals. Shown are exemplary results of left triceps surae (LTS) at interstimulus intervals of 30, 50, and 100 ms derived from an individual with chronic incomplete spinal cord injury. DOI: 10.1007/978-3-319-72736-3_33
This is the response to a single stimulus (B) or two stimuli (C) at different interstimulus intervals. This is expected when we stimulate, the muscles give us a response to the applied stimulus at a certain amplitude. The way these muscles respond tells us if we’ve properly placed the electrodes. If a certain group of muscles (proximal or distal) are not responding or giving a very minor response we can move the electrodes up or down the spine to better stimulate the area we are interested in.
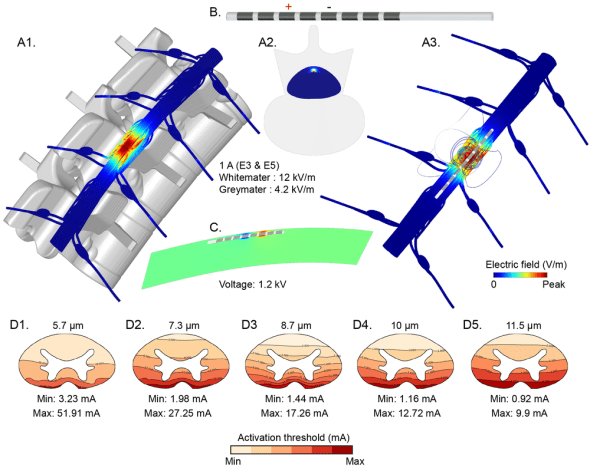
In the image above (A) we see how the electrodes are placed, one electrode (cathode) goes on the spinal cord in the area we want to stimulate and there are two (anode) electrodes placed on the front of the body around the stomach area (normally the iliac crest, but here they used the stomach, which to me seems uncomfortable). This is because electricity flows from the cathode (stimulus) electrode to the anode electrode, so we need to place the electrodes in a way that activate the spinal circuitry. If for example, we place the anode electrodes on or near the spine, we won’t get the penetration we need to stimulate the cord because the stimulus will travel along the skin to the anode electrode. We may stimulate some of the surface muscles along the spine, but we will not end up stimulating the cord itself.
How does the spinal cord respond to stimulus when we have someone walking? This is the main use for spinal stimulation (to restore function) and like we’ve seen in the presence of stimulus, the threshold for the circuitry to fire is lowered, so in the presence of stimulation we have an increased volitional response! Below is an EMG recording of several muscle groups while a person with spinal cord injury is walking unaided (left) and in the presence of stimulation (right).
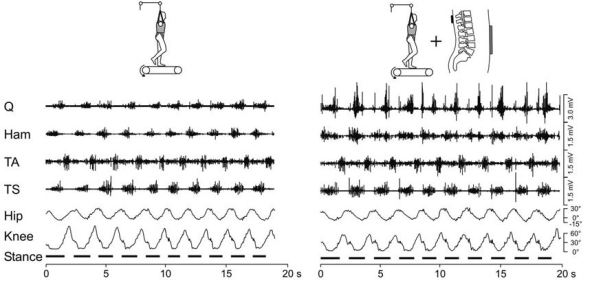
Supported person with spinal cord injury walking unaided (left) and in the presence of spinal stimulation (right). Notice that the EMG response in the presence of stimulation is much higher than unaided.
We’ve posted this video before, but it’s worth sharing again. Below is a video showing a person laying on the side (supported) trying to walk unaided, then again under the presence of TSS. You’ll notice that the response is dramatically different and this is completely volitional, no one is moving the persons legs other than the person themself. The attachments you see are used to support the weight of the legs while they hang off the bed.
That gives us a look at how TSS stimulates the spinal cord and why we use it over epidural spinal stimulation. While there is still a lot to figure out about the technique, it’s already doing some amazing things and it is non-invasive making it a great tool for research as well. As you might be able to tell, it’s all very exciting to me and I hope that I’ve gotten you excited about it as well!
Until next time, don’t stop learning!



But enough about us, what about you?