Know your spinal cord – Invasive spinal stimulation techniques
It’s day forty-six in our spinal cord series. While we’re nearing the end (maybe), there are still a few things to cover. First, if you’re new, you can find all of the posts in the neuroanatomy category for when you need a quick spinal cord fix. I’ve been debating about this post for some time, but I figure we might as well cover it since we’re here. Today we are going to talk briefly about invasive spinal stimulation and what the future might hold.
The spinal cord is delicate. That is probably an understatement. It’s basically pudding, it will deform under its own weight! The brain is the same way, so never fear the body does a great job of keeping them protected and supported (thanks body). However as humans we are not content with letting the body be in charge, we want to fix injury, or birth defects, or maybe just improve the quality of life for people. These two things, seem somewhat unrelated, but really because of how delicate our tissues are, the interfacing part is very difficult.
Brain machine interface, the final (or maybe first) step in our own self directed evolution. We have the technology, but we don’t have the materials. The issue is how we are trying to interface, if we use a really soft material, we cannot get it to penetrate easily into the brain/spine/whatever. On the other hand if we use a very rigid material we have to deal with it tearing into the tissue, deforming it, and possibly scaring to the extent that it no longer records any signal. That is why we are having such a hard time taking that step.
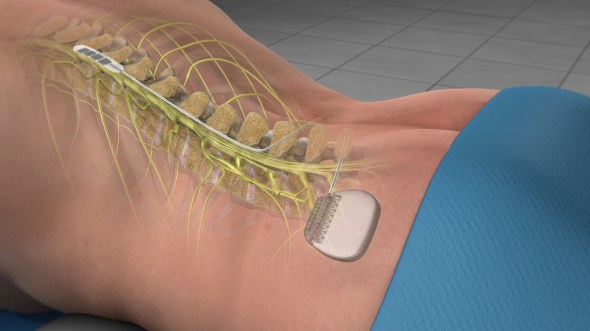
Spinal stimulation sort of works around this because it does not need to penetrate the cord. It just sits in the epidural space, so as long as it isn’t blocking or pinching, it can hang out indefinitely. However, just like brain-machine interface, we would like to be able to penetrate the cord to stimulate a very specific region. First let’s look at what we normally use in epidural spinal stimulation. Below is an image showing several different style of lead. They all have the same basic structure and have multiple electrodes (the dark spots) to give some ability to adjust the region of stimulation.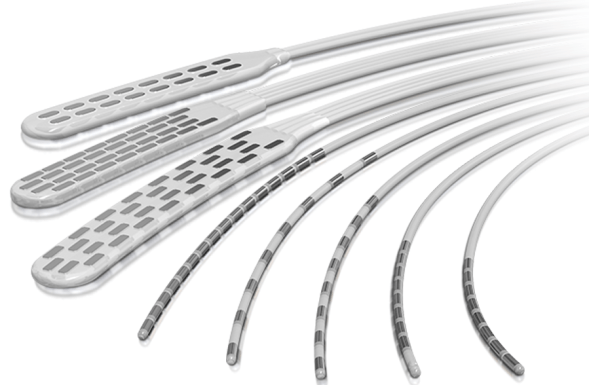
In terms of technology this is as basic as it gets. There is a lot of things that go into the design, creation, material properties, etc. don’t get me wrong, it is a very impressive feat of engineering, but it would be like comparing technology from the 60’s with technology of today. We’re still very much stuck in the early stages of this type of treatment.
More recent advancements are still being made using animal models. For example we’ve implanted a utah array into a rat spinal cord and it works… for the most part. Unfortunately, it deforms the cord after time and there is scaring to work out. This is a material properties issue for sure, but also a biological problem that we need to find a way to work with or sidestep all together. Below is a drawing showing how this electrode is placed and it gives you an idea of the size of the array as well as its shape.

The most advanced option would be to separate the array so instead of one solid piece you have small wires inserted. This is the idea behind neuralink and would also work with spinal cord stimulation. Below is an image of such a setup, once again tested on a rat model. This did not deform the cord and there was far less (although still present) scaring.

Overall the technology still has quite a bit of work before it is something that will be used in a spinal cord injury population and this is super invasive, so the research needs to mature first before we can get to even thinking about first in human trials. It’s quite a ways off, but looking at the work being done now gives us a good idea about what may be coming in the next 10-15 years.
Until next time, don’t stop learning!



But enough about us, what about you?