Know your spinal cord – Spina bifida
This is day nineteen of knowing your spinal cord! We covered all the big neuroanatomy and while we may go back and cover some of the minor things, we’re in the middle of spinal deformities. For those just starting, we have a neuroanatomy category to make it easy to find these posts. For everyone else, today we’re talking about spina bifida.
For the past few days we’ve looked at some uncommon spinal deformities. In contrast, spina bifida is unfortunately much more common. Spina bifida is the term for an incomplete closing of the spinal membranes around the spinal cord. There are three distinct subtypes of spina bifida and we’ll cover each one in order of severity.
Spina bifida occulta
First let’s talk about spina bifida occulta. Occulta is latin for “hidden,” and this is the mildest form of spina bifida. This is a somewhat special case of spina bifida when compared to the others. In this case, the vertebra haven’t fully formed. Like with diastematomyelia, it occurs mostly on the lower back (lumbar), in fact all types of spina bifida commonly occur in the lumbar region, although as with diastematomyelia it can uncommonly occur in other areas such as the cervical area.
Out of the three types of spina bifida, you cannot really see it outside of the body. In fact, most people who have this type of spina bifida are asymptomatic and don’t know they have it. Out of all the types of spina bifida, this type accounts for about 15% of the cases. This number COULD theoretically be higher, but we may not know becuase of the nature of the defect. There are certain blood tests that can be used to screen for spina bifida, however this type will not show up on the test because it tests for a high AFP, a protein that does not increase due to this type of spina bifida.
Spina bifida meningocele
This is a more severe form of spina bifida and can be seen due to the meningeal cyst that forms in the area on the back. This is the least common form of spina bifida and is characterized as a single developmental defect that allows themeninges to herniate between the vertebrae. However, the spinal cord remains it’s normal location, the third type of spina bifida we will cover makes this distinction. Therefore, because the nervous system remains undamaged, individuals with meningocele are unlikely to suffer long-term health problems, although cases of tethered cord have been reported. This is likely due to the tethering of the meninges and the pull it creates on the cord.
Spina bifida myelomeningocele
Lastly we have myelomeningocele, the third and most severe form of spina bifida, it is also unfortunately one of the more common forms of spina bifida. This too presents with a meningeal cyst, the difference between this and meningocele is that the unfused portion of the spinal column allows the spinal cord to protrude through an opening. In this case the cyst holds not just spinal fluid, but the actual spinal cord and/or nerves. This typically occurs in the third week of fetal development, but thankfully it can be tested for.
Technically there is a more severe form of myelomeningocele called myelocele. So really there are four types of spina bifida, but this is usually lumped with myelomeningocele. In this case, just like myelomeningocele, you have a meningeal cyst with the spinal cord and/or spinal roots inside. However, in this form, there is nothing covering the mengies, no skin whatsoever; they are completely exposed to the world. As you might imagine, this can cause infections like meningitis, which can be life threatening.
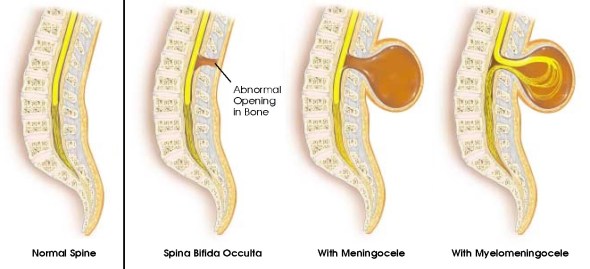
We know that there is a genetic component at play, as well as environmental factors. Girls are more at risk than boys, those who are white or hispanic are at a higher risk than other ethnicities. However, the details of why this happens are still to be determined. Below is an image that shows the three major types of spina bifida.
One of the things we research in our lab is how to help rehabilitate individuals with spina bifida. This is because most commonly they cannot walk normally. However, with physical therapy this can be improved. Most commonly children and adults with spina bifida have weakness in the lower extremities. They also can have orthopedic abnormalities such as clubfoot. Because people with spina bifida have an abnormal gait, we try to help with physical therapy such as orthotics, but more recently we are turning towards assistive exoskeletons.
In this a rehabilitation role, the exoskeleton would provide assistance and not fully function for the person. This helps teach the spinal cord (because we can do that) and helps strengthen muscles that are sometimes underdeveloped. This can be further exacerbated when left untreated because people will compensate for foot drop by hiking the hip upward, thus creating a muscle imbalance and again training the spinal cord to walk in this abnormal gait.
That wraps up your introduction to spina bifida. Stick around for more interesting spinal knowledge. As has been the theme the past few days, I’m not sure what we will be discussing tomorrow, but I will make sure that it is something very interesting! So stick around, it will be fun.
Until next time, don’t stop learning!



But enough about us, what about you?