Day 224: Review – Cortical and Subcortical Effects of Transcutaneous Spinal Cord Stimulation
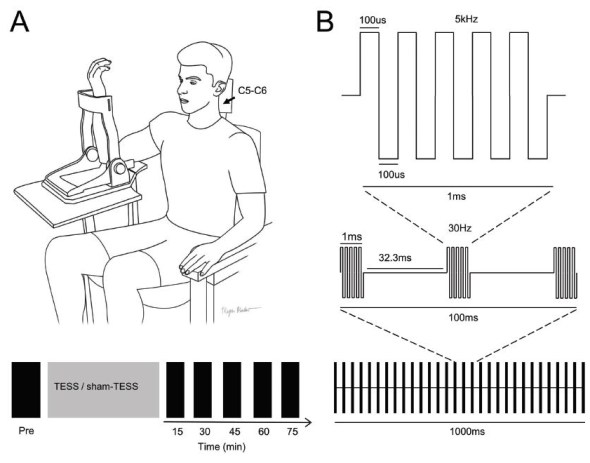
Experimental set-up. (A) Participants were comfortably seated in a customized chair during transcutaneous electrical spinal stimulation (TESS) or sham-TESS for 20 min. TESS was delivered using a surface electrode on the back of the neck between C5–C6 spinous processes segments (cathode) and a surface electrode in each anterior crest of the hip bone (anode) using a custom made 5 channel stimulator (BioStim5, Cozyma). Electrophysiological and behavioral outcomes were tested before (Pre) and immediately after, 15, 30, 45, 60 and 75 min after the end of the stimulation or sham stimulation period. (B) Schematic representation of the type of current used during TESS. We used 5 biphasic pulses at 5kHz with each biphasic pulse lasting for 200us. The middle scheme shows the blocks of 5 biphasic pulses passed at a 30Hz frequency. Lower part of the schematic shows the number of pulses delivered in one second.
Well it’s been two weeks since the last critical review so it’s that time again. As usual, my PI gets a copy and so do all of you. Since I’ve done several of these now (this is number six) I have a category just for these reviews called critical reviews. This is a really new study which tries to help tease apart what we are actually stimulating when we apply transcutaneous spinal stimulation. I think it’s a super interesting paper and I hope you do as well.
Transcutaneous spinal stimulation (TSS) has been shown to promote functional recovery for people with spinal cord injury (SCI). However, the mechanisms by which TSS works are still poorly understood. While it has been made clear that TSS pulses pre-activate spinal networks the effects of repeated use of TSS on the central nervous system pathways remains unknown. By better understanding the neural mechanisms behind TSS-induced recovery, we will likely be able to improve rehabilitation effectiveness. The researchers of this study hypothesize that TSS has a predominant excitatory effect on spinal networks while providing a predominantly inhibitory effect at the cortical level.
After 20 minutes of either TSS or a sham-TSS applied between the C6-C7 spinous processes, the researchers used motor evoked potentials (MEPs) and cervicomedullary evoked potentials (CMEPs) stimulated using magnetic stimulation. They measured the electromyographic (EMG) response at the triceps brachii, biceps brachii, and the first dorsal interosseous (FDI) muscles to determine the affected pathways. Measurements were taken at 15, 30, 45, 60, and 75 minutes after intervention and done on the right side for the control group and the less affected side for the SCI group.
TSS was applied in blocks of five 200 µs biphasic pulses at a frequency of 30 Hz with a carrier frequency of 5kHz. A second condition used the same parameters but eliminated the carrier frequency (TSS w/o 5 kHz). The sham stimulus used the same location and amplitude, but the amplitude was gradually reduced over the course of ~1 minute to zero. The study had 17 subject who had a chronic SCI (> 1 year since injury) with 15 age matched healthy control subjects. Subjects performed 2 elbow flexions at maximal voluntary contraction for 3-5 seconds with a 30 second rest. Functional outcomes were also measured using a fine motor tasks which included jar opening, water bottle test, a key test, and a coin test.
Analysis of the results was done using a repeated-measures ANOVA and found that intervention (TSS) increased CMEP amplitudes in both the healthy and SCI groups for measurements taken at 15 – 75 minutes, but no difference in MEP amplitude. They also found that short interval intracortical inhibition (SICI) increased for 15-75 minutes after TSS. For TSS w/o 5 kHz the results were similar to the TSS findings; however, MEP amplitude increased with TSS w/o 5 kHz at all measurement points (15-75 minutes). The authors state that this suggests the 5 kHz carrier frequency has a suppressive effect on corticospinal excitability. For functional outcomes they found that the mean time to complete the tasks dropped after both TSS and TSS w/o 5 kHz. However, the decrease in time was larger for TSS than with TSS w/o 5 kHz.
Overall the researchers concluded that TSS can change excitability of cortical and spinal networks in both healthy and SCI populations. What was particularly interesting was how the researchers used both a TSS and a TSS w/o 5 kHz carrier frequency to determine if the carrier frequency influenced the activated networks. Because the standard parameters for spinal cord stimulation are selected based on years of finding the subjects responses to stimulation, we still don’t understand why or even if those parameters are optimal. Findings like this help us better understand why certain stimulation paradigms work better than others and offer insight into ways we can modify those parameters for different desired outcomes.
Source:
Benavides, Francisco D., et al. “Cortical and Subcortical Effects of Transcutaneous Spinal Cord Stimulation in Humans with Tetraplegia.” Journal of Neuroscience (2020). DOI: 10.1523/JNEUROSCI.2374-19.2020



But enough about us, what about you?