Effects of transcutaneous spinal stimulation on spatiotemporal cortical activation patterns
It’s official! My latest paper, what I’ve been calling “last paper” is now typeset and I can share my fancy videos better. I’m excited that this is finally here and since I gave a good overview of the paper (here) today I’ll discuss a bit more about why this paper was important and why the dataset was such a pain, both of those I had to shorten due to the length of the post.
So first off, this paper took so long because I had to learn a ton of new skills and the dataset itself was super noisy. I think I mentioned that EEG (more here) is incredibly sensitive, on order of a microvolt or 0.000001 volts! Very tiny and the sensors we use for EEG are prone to artifacts from just about anything a person does from movement to eye blinks! Even if we assume the person closes their eyes (sometimes we do this), the eyes still move in the socket, which (you may have guessed) causes a lot of electrical change that the sensors pick up. EEG is so sensitive that we can pick up electrical interference from the lines in the walls, called line noise which is 60 Hz here in the US.
Now transcutaneous spinal stimulation (TSS) involves using electrical current delivered over the skin over the spinal column to activate the dorsal roots of the spinal cord (more here). That’s just a fancy way of saying the nerves that enter the spinal cord (because there are nerves that go in and come out defined by the direction of the signal) become activated and activate circuitry in the spinal cord, which can in turn cause movement. It’s really cool, trust me on this. We can do this two ways, TSS is the non-invasive way and there’s another invasive way called epidural spinal stimulation (ESS) which requires surgery to insert the leads into the epidural space (space surrounding the spinal cord).
ESS is handy because we can target specific spinal nerve roots, which we can do somewhat with TSS, but it’s not nearly as specific. The other major difference is the amount of current needed. Because TSS needs to go through the skin, muscles, fat, etc. it requires on order of 10x more current to go above motor threshold (threshold for a muscle response). Almost all electrical stimulation (aside from very low amplitude and/or stimulation far away from the recording electrodes) will leave an artifact. It’s nothing more than the change of the current on the skin due to the stimulus and because it’s traveling over the skin it (for all intents and purposes) is instantaneous.
If we only applied a single stimulus this wouldn’t be a problem, we could align the responses using the stimulus as time t = 0 (which we actually did in the paper), and you could see the effect of the response to the stimulus (in my case on the brain). However, we were interested in continuous stimulus, depending on the task we applied either 30 or 15 Hz (30 Hz is 30 electrical pulses a second!) for the entire time the task was being done, thus a very noisy dataset!
Dealing with these artifacts turns out to be very difficult. Which is one of the things I’ve learned over the course of working on this paper (see: years, with an s). I ended up using independent component analysis (ICA) to find the “pure” sources instead of what we get from EEG which is mixed sources. Imagine you are recording conversations inside a restaurant by surrounding the outside of the building with microphones, that’s basically EEG and the inside of the restaurant is where the brain is. Each person talking inside the restaurant would be a single source and ICA can break apart the mixed sources and return individual conversations. It’s not perfect, there are limitations, and there are assumptions we need to make, but it does a great job.
By doing this for each subject and using something called dipole fitting, we had the individual “conversation” AND the location! Basically dipole fitting determines where the IC (independent component or “conversation”) using the forward model meaning we know the electrical properties of the tissues the signal travels through so we can use our recording to estimate the location (paper for those interested in learning more). Both the forward model and inverse model (using source information to determine what we should see at the sensor) have solutions, but the inverse model is ill-posed meaning there are (basically) infinite solutions, so we typically use the forward model. Again limitations and assumptions apply, not valid in the state of wyoming where physics is against the law.*
*not a real thing
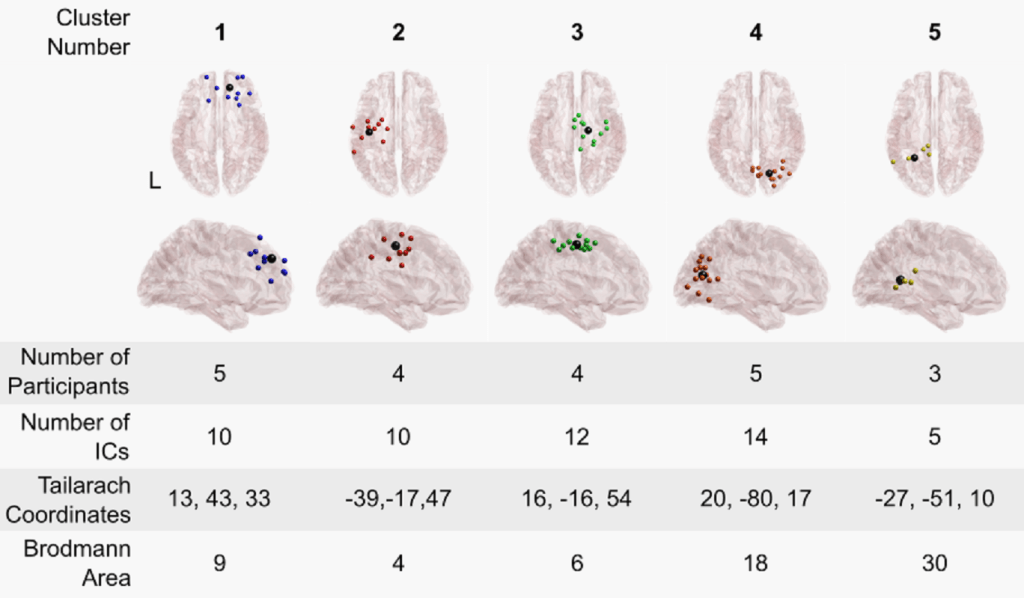
Then we clustered the data across subjects, that is looked at the dipole locations for everyone and found common areas of activation. We found five and the video shows how they interact! Because we had several different types of conditions the video (at the bottom) is the rhythmic contraction (RC) task (pseudo-walking) and it shows the difference in the alpha band (specifically, we have the others located in the supplementary materials of the paper) between the RC with stimulation and RC with no stimulation tasks. Only significant differences are shown (corrected for multiple comparisons).
So why was this important?
Well we establish a baseline for the average neurologically intact person. More importantly, we’ve shown that TSS does cause changes in the brain, we’ve determined where those changes are located, and we hypothesize why those changes occur. This actually supports some of the findings from a previous paper I authored (this one), where we suggested that the brain doesn’t really tell the spinal cord to move the leg. Instead it releases a control it places on the spinal cord and it lets the spinal cord do its own thing!
This is an interesting hypothesis because it means the spinal cord is largely in control of movement — at least in the lower limbs — which is far away from the brain neurologically speaking the delay is ~30 ms or so, which is a loooong time neurologically speaking! It somewhat makes sense because we really don’t need to focus on walking and the circuitry exists to control walking (see: the central pattern generator), at least in animals, but we expect humans have one too.
This also has implications for rehabilitation after spinal cord injury (SCI). When SCI occurs, in a lot of cases the circuitry for walking (the lumbar enlargement) remains intact, the only change is that the brain can’t send signals to it to cause movement. Since most SCI (99.9% really) is not a complete break, there’s still signal being sent, it’s just not strong enough to cause movement. This is why TSS and the invasive ESS are being looked at for rehabilitation and restoring function.
This paper helps put the pieces together to help determine better ways to stimulate. It also opens the way for using TSS and EEG as a way to probe spinal circuits after SCI to determine the changes after SCI and how communication is affected. This is important because the average years of remaining life after SCI has not improved since the 1980’s meaning if you got hurt in 1980 your life expectancy afterwards would be roughly the same as if you got hurt today (source).
That simple statistic has a starling message behind it and it’s simply that, what we are doing is NOT working. So we need to find different and better ways to help treat SCI. The spinal cord is a complex beast, we barely have an understanding of how it works besides the superficial stuff (how it’s constructed). We need to learn how it works and this paper is a step forward to a world where we can understand the language of the spinal cord. Once we figure out how to better “talk” to it, we will be able to do some incredible things and I’m excited to help build that future.
My dear readers, forgive me for indulging my paper once again. This has been years of work and I’m very proud of the outcome. While I think things could have been done differently/better, I’m very happy with our result and I do look forward to getting to try to improve upon the methodology in the future. I learned a lot over the past few years and I sincerely hope that comes across in the paper and my discussions about it.
As always, thank you for joining me on this journey. Your support has been a literal live saver for me. Oh and I’ve got more big news on an old topic which I’ll share tomorrow, so you’ll need to forgive me in advance for that as well (assuming I post what I think I will).
Source:
Steele, Alexander G., et al. “Effects of transcutaneous spinal stimulation on spatiotemporal cortical activation patterns: A proof-of-concept EEG study.” Journal of Neural Engineering (2022). 10.1088/1741-2552/ac7b4b



I don’t think it’s any problem that you’re talking about the paper a second time! It’s a bit of a weird feeling to sink many hours into a project, get a result, show it to the world, and then think “is that all?” as the publicized output slips away in the stream of internet noise. Go ahead and drag it out a little bit – it’s worth that.
Now that I can see the neat video, I notice that the change in information flow between the different brain regions doesn’t appear to track the roughly sinusoidal contractions. E.g. there’s no identical set of arrows that appears every time the right ankle is at maximum, or anything like that. Why do you think it’s so variable?
I keep on being wowed by the possibility that my spinal cord does a lot of the basic motor control by itself, and the learned motor sequences aren’t just in my cerebellum like I learned in elementary school.
Now that I think about it, have either of your labs ever tried doing EEG on the cerebellum? The internet suggests to me that it’s difficult.
LikeLiked by 1 person
July 1, 2022 at 10:28 pm
Thanks, I sometimes worried that posting more than once or twice on the same topic makes it seem too repetitive and/or attention seeking. But yeah there’s years of work in this paper so it does feel nice to be able to visit it a few times.
When I calculated gPDC I used a 2 second window with a 1 second step size (so roughly 1 second differences). So we couldn’t really “see” effects from a single movement, more like overall changes for that time window (that you see at the bottom). It’s a limitation of the technique. We could (in theory) use different sized windows for different bands, but then we couldn’t compare across bands (in my opinion anyway).
Right? It’s sad, but we (science) has studied a lot in decerebrated cats and other animal models and they can still walk when we activate the cord the right way. We expect humans are the same (have a CPG), but we don’t know for sure. It does mean that we could (in most cases and in theory) restore walking in people with SCI though. Maybe one day… hopefully one day sooner rather than later.
The cerebellum for EEG purposes would be considered a “deep brain structure” so yeah hard to do with EEG, but we do MRI studies and look at what’s going on in the cerebellum and brainstem since there’s not a depth limitation with MRI.
LikeLiked by 1 person
July 2, 2022 at 10:45 am
Hi there,,
I am not sure if I will get a response, but let me give it a try!
I found your website accidentally during a google search, and I loved the content and the spirit of this (diary/journal?).
I found your post, and then your paper on Source-Modeling of EEG Data Using EEGLAB and Brainstorm.
I am new to source modeling, and I didn’t use brainstorm before (I am decently good with EEGLAB scripting).
Ah, anyways, I am trying to replicate your pipeline on your own data, before I try to implement it on my data (a motor imagery experiment).
Your pipeline has 7 steps. I was able to follow the first 5 successfully.
Then we have visualization, steps 6 and 7. I am interested in TF analysis and this is why I moved to step 7. However, it seems I am stuck there.
Do you think you can help me with this? Maybe over zoom if you kindly agree? I know it is strange – a stranger asking for a bold zoom help.
Anyways, thanks for the nice post, pipleline, and work 🙂
LikeLike
December 6, 2024 at 1:27 pm
Hi, I should probably be better about keeping up with my blog! I’m glad you liked it and the pipeline. The visualization steps are a bit tricky, so I can understand why you may be stuck and I would be happy to help if you still need it. I’m totally fine with a zoom meeting if you would like, it’s the least I can do to help a fellow researcher. I’m emailing you after I post this response, so if you don’t see it, just respond here and I’ll reach out again. Thanks!
LikeLike
December 20, 2024 at 11:39 am
Thank you so much for taking the time to respond to my comment! I did receive your email and I responded back with questions and possible way to connect. I hope we are able to discuss very soon!! 🙂
LikeLike
January 13, 2025 at 2:41 am